



Participants
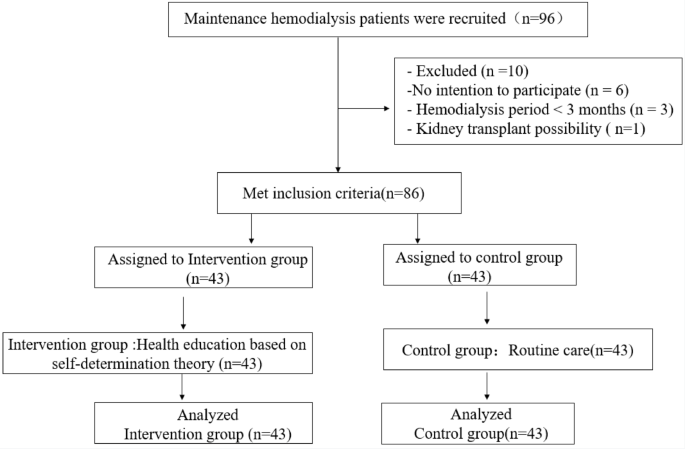
The research was a quasi-randomized control trial. Eighty six MHD patients admitted to a tertiary hospital in Deyang City from June to December 2023 were selected according to the inclusion criteria: (1) age ≥ 18 years, meeting the diagnostic criteria of end-stage renal disease in K/DOQI guidelines20; (2) hemodialysis treatment time ≥ 3 months, 3 times/week, 4 h/session; (3) signed informed consent. Exclusion criteria were: (1) unstable condition or combined with other serious diseases; (2) history of mental illness; (3) a possibility of a kidney transplant in the near future.
Sample size: the sample size was calculated using the formula:n1 = n2 = 2[(Zα + Zβ)σ/δ]2, Taking bilateral α = 0.05, β = 0.1, checking the table, we get Zα = 1.960, Zβ = 1.282, according to the literature research results21, based on the calculation of MHD patients’ self-management scores, δ = 8.7, σ = 11.2, it comes out that n1 = n2 = 35, and considering 10% to 20% of lost follow-up, therefore, the actual sample size of 86 MHD patients was calculated.
Hemodialysis nurses invited patients who met the inclusion criteria for this study after being fully informed of the aims and procedures. Forty three patients who were dialyzed on Monday, Wednesday and Friday were in group A. Forty three patients who were dialyzed on Tuesday, Thursday and Saturday were in group B. Groups A and B were randomly divided into the intervention group and the control group by using the method of flipping a coin, and all of the 86 people completed the three months of the intervention study. Figure 1 shows the Flowchart of the study.

Setting
The control group received routine care, including health education manual, centralized education, bedside individualized guidance and telephone follow-up during dialysis. Concrete content included hemodialysis knowledge, exercise, diet, fluid intake, vascular access maintenance, complication prevention and medication knowledge. Centralized education was carried out in the health education room of the department, the individualized guidance session was conducted during hemodialysis treatment in the hemodialysis center.
Intervention procedure
The intervention group received health education based on self-determination theory. (1) Establishment of intervention team: a nurse manager, eight hemodialysis specialist nurses, two clinicians, a dietician, a psychologist, and the members of the intervention team receive homogeneous training. (2) The doctors conducted collective health education for the patients in the intervention group in the form of PPT (once a month, 45 min/time). The specialist nurses evaluated the health education content received by the patients through the way of scenario simulation, and gave small gifts to the excellent evaluation. (3) Individual guided interviews (four times, 20 min/ time): ① Autonomy needs: understanding the patient’s disease process, guiding the patient to express positive or negative emotions and acknowledge the patient’s point of view; listening to the patient’s experience of self-management, guiding the patient to draw the weight gain curve in the last 2 weeks; encouraging the patient to talk about the important things in his/her life and hobbies, etc.; the dietician take into consideration the patient’s financial ability and dietary preferences, etc., working with the patient to develop a home diet plan list. The doctor in charge develops an individualized exercise program with the patient according to the patient’s exercise preferences and habits. ② Competence needs: guiding patients to formulate practical and progressive goals and plans, exploring possible obstacles in the implementation process, and assisting patients in finding solutions; using food models as teaching aids to guide patients to master the estimation of food water content, as well as cooking to reduce phosphorus and soaking to reduce potassium, and other interventions such as micro-telephone groups, one-on-one telephone follow-ups, and self-monitoring diaries to ensure the sustainability of the implementation. Sustainability. ③ Relationship needs: encouraging patients to express their own feelings, giving psychological support and channel bad emotions; encouraging patients to communicate with bedside patients during the dialysis process; advocating family accompaniment, and it is best for family members to participate in and supervise the whole process of behavioral change, so as to increase the patient’s sense of family belonging needs.
Pre-specified primary and secondary objectives (hypotheses)
Primary objectives (hypotheses)
Explain program’s efficacy (Improve the hemodialysis knowledge level and self-management behavior of MHD patients).Hemodialysis Related Knowledge, measured using the Hemodialysis Related Knowledge Scale. Self-Management Behavior, measured using the Self-Management Behavior Scale.
Secondary objectives (hypotheses)
Decrease adherence difficulties (interdialytic weight gain) and mental difficulties (anxiety and depression).Interdialytic Weight Gain (IDWG), measured using the average value from the 3 most recent dialysis sessions. Anxiety and Depression, measured using the Hospital Anxiety and Depression Scale.
Examine change in knowledge /self-management behavior as a mediator of the effect of a health education program on mental health and adherence difficulties.
Measures
Hemodialysis related knowledge scale
The Hemodialysis Related Knowledge Scale developed by Curtin22, the scale was translated, modified and culturally adjusted by scholar Li Hui to form a Chinese version of the hemodialysis related knowledge scale23. The scale included diet, medication, dialysis treatment, rehabilitation nursing and other subject categories, with a total of 24 items. Correct answers were counted as 1 point, and incorrect answers or ignorance was counted as 0 points. The score range was 0–24 points. The Cronbach’s alpha coefficient was 0.701.
Self-management behavior scale
The Self-Management Behavior Scale developed by Li Hui and was used to evaluate the level of self-management behavior in hemodialysis patients24, including four dimensions of partnership (4 items), executive self-care (7 items), problem solving (5 items) and emotional processing (4 items), with a total of 20 items. The scale adopts Likert 4 scoring method, assigning 1–4 points, ranging from 20 to 80 points. The higher the total score, the better the self-management behavior of MHD patients. The Cronbach’s alpha coefficient was 0.862.
Interdialytic weight gain
Interdialytic Weight Gain (averaged from the 3 most recent dialysis sessions) was calculated as the average change in weight between dialysis sessions25.
Hospital anxiety and depression scale
Hospital Anxiety and Depression Scale (HADS) was developed by Zigmond and Snaith in 198326 , including two subscales of anxiety (Anxiety-Symptoms, HADS-A) and depression (Depressive-Symptoms, HADS-D), each with 7 items, and a total of 14 items in the total scale. Likert 4 scores were used for this scale, ranging from 0 to 3, and the total score ranged from 0 to 42. The higher the score, the more serious the degree of anxiety and depression. The Cronbach’s alpha coefficient was 0.890 for the total scale and 0.820 and 0.807 for the anxiety and depression subscales.
Data analysis
SPSS version 26.0 (IBM Corporation, Armonk, New York, USA) were used to analyze the data, Count data were expressed as frequencies and percentages. Mean and standard deviation (\(\overlinex\) ± s) were used to describe continuous variables. Chi-square test (χ2) was used for comparison between groups. 2-Independent-samples t test was used to compare the two groups before and after intervention. All statistical tests were conducted by two-sided tests, with differences considered statistically significant at P < 0.05.
Ethical consideration
The study followed the principles of the Declaration of Helsinki, informed consent was obtained from the patients and their families before the start of the intervention, and the project was reviewed and approved by the Ethics Committee of Deyang People’s Hospital (Ethical number: 2022-04-030-K01). Health education measures based on SDT were also conducted in the control group at the end of the study.
link